Before the change
CETENA was hired to conduct the HF assessment of a ship design that the Client was carrying out. Unfortunately when the activity started the Client had already completed the basic design phase and could not substantially modify it despite the suggestions made. In fact, their ship had some flaws from an ergonomic perspective.
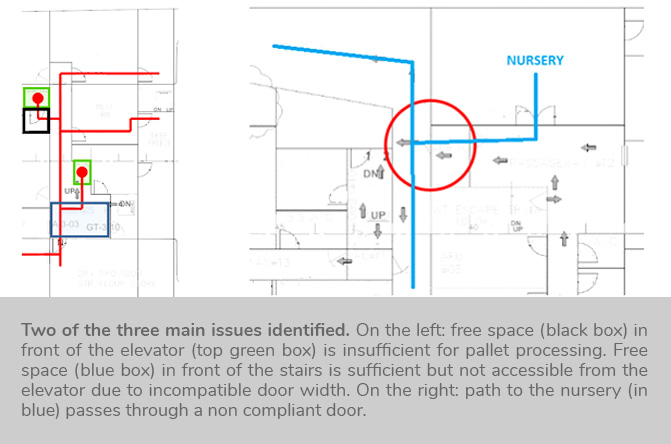
Three main issues were identified:
1)In front of the food stores, there was no free area for the transpallet to turn, so the operator could easily get stuck and he had no place for dismantling the pallet before fitting provisions in the stores. Moreover, the width of the elevator door was exactly the same as the width of the transpallet used to fetch the provisions, another aspect leading to potentially serious problems due to the missing clearance.
2)Analysing the path from the top deck to the nursery, it was pointed out that the path had a very big flaw, i.e. a very sharp bend between two corridors that made it very difficult for people carrying a stretcher to make the sharp turn. The difficulties are due to the stretcher’s length and the fact that carrying an injured person greatly limits the movement the stretcher can have. For completing the transportation, the patient has to be lifted at weird angles in order for the stretcher to make the turn.
3)The location of the lifts for ammunition stores was analysed. Ammo pallets are delivered on the top deck by a crane and then a lift is required to take the pallets to the ammunitions stores. If the lift doesn’t work then the ammunitions boxes need to be taken to the stores by hand, dismantling the pallets on the top deck itself. The ship had a really long way to reach the ammunitions stores that made it impossible to complete the operation by hand in a short time and without excessive fatigue to the operators, due to the fact that the Client did not properly take into account guidelines on hand transportation, leaving it to operative crew members on-board. This aspect is quite typical when evaluating designs carried out by shipyards of emergent economies, where society stratification is more pronounced and the greatest part of the attention is on Officers comfort, while lower ranks are usually less considered.
After the change
The aforementioned issues were pointed out paying attention to include indications on how to improve them.
1) Free area in front of the food stores: it was simply suggested to increase the available area and to enlarge the lift door.
2) Sharp bend between two corridors in the path to the nursery: it was suggested to increase the corridor opening to ease the manoeuver when carrying the stretcher. A specific habitability guideline exists on this issue in Fincantieri guidelines database:
[Hab. 3.136]
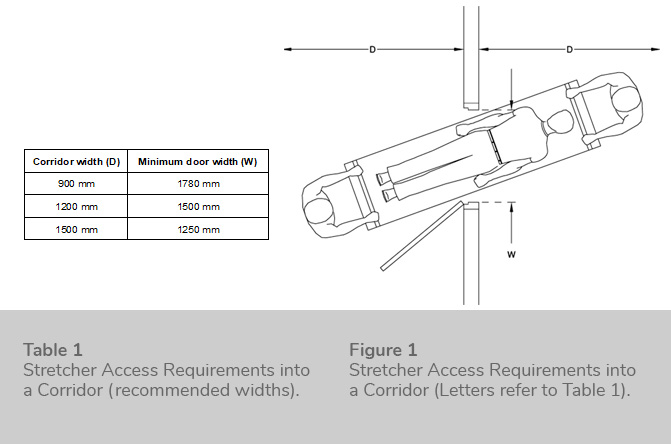
The minimum door width for access with a stretcher directly into a corridor at right angles to the door depends upon the width of that corridor. Table 1 and Figure 1 show the door width required to move into different widths of corridor without unduly tipping a stretcher.
Location of the lifts leading to ammunition stores: the Client understood the flaw but there was no way to solve it and accepted the operativity reduction counting on the massive available workforce on-board to complete the ammunitions loading operation in a finite time.
Overall, it is unknown whether the Client did any changes based on the analysis. However, they learned the process for integrating HF requirements at design phase and understood the implications of overlooking HF aspects and trying to solve them in a more advanced phase. Moreover, the consequences of developing a ship design that satisfies higher ranks needs despite a decrease of comfort for lower ranks was pointed out, and used as the main argument for explaining the inefficiencies and the lack of effectiveness of the design.
How and Why
This methodology is normally applied in Fincantieri Group and goes by the name of Flow Analysis, an effective tool for evaluating the design of a ship from a general perspective. A ship is a very complex environment, where hundreds of people interact and carry out possibly conflicting activities. The majority of physical-related activities involve movement (e.g. moving from one compartment to the other to perform maintenance, carrying materials with transportation tools, queuing for lunch, reaching the area of operations for safety reasons, etc), an activity onto which the topology of the ship and the placement of compartments has a huge impact. The usual procedure for such a study requires looking at the general arrangement while defining a block diagram that follows closely the movement of goods or people. Then, for each block the HF expert has to detail basic questions like what, when, who, where. In this simple way knowledge is gained on how the designer intends to plan the activity and critical steps are easily identified. A strong knowledge of best practices, international standards and generally speaking experience on the field is absolutely mandatory, since the ergonomist must warn the designer on the overlooked aspects and motivate the importance of the identified gaps.
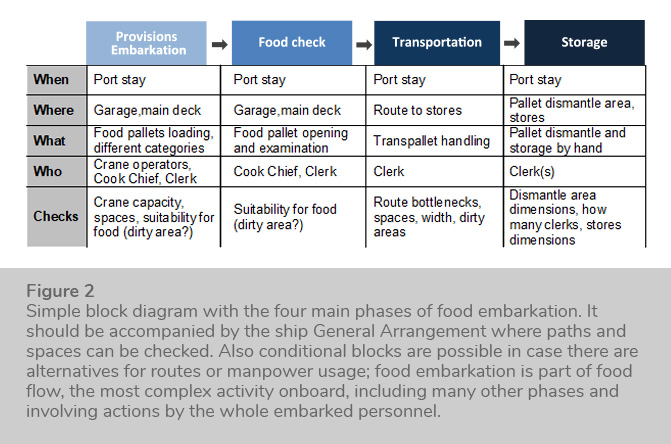
Usually these activities are done for a variety of ‘flows’, including
-Food flow (provisions embarkation, preparation, consumption, waste disposal, etc)
-Ammunitions handling, from main deck to ammunitions stores including weapons refilling activities
-Safety teams operations, where it is demonstrated that safety teams can access every part of the ship while wearing bulky protective clothes
-Evacuation routes with a qualitative evaluation of bottlenecks (to be refined with an actual software based evacuation study if requested)
-Injured personnel recovery (access to nursery, bottlenecks free paths)
The flows also depend on the kind of ship operation and may include CAD verifications for fine aspects (e.g. manoeuver spaces for a fork lift inside a store can be checked geometrically). This HF assessment can be done at any stage of the design/build process of the ship but it can result in actual improvements only if it is performed during the basic design phase. If done in other phases, most probably the suggestions will not be followed due to the many constraints on ship compartments dimensioning and positioning.